

What is an Epidural for Labor Pain?
Using an epidural in labor pain is widely known as a method for pain relief during labor and birth. An epidural is an anesthetic (and sometimes a narcotic as well) placed directly in the spinal column to block sensations from the lower half of your body. Epidurals are widely used and, when they work as intended, are the most complete form of labor pain relief available. When birthing in hospitals where epidural anesthesia is available, the percentage of its use is very high.
If you think your pain tolerance is low, you may be considering an epidural for labor pain. However, there are quite a few ways to lower your experience of pain without the risks of an epidural, whether or not you’re keen on natural childbirth.
How Does an Epidural For Labor Pain Work?
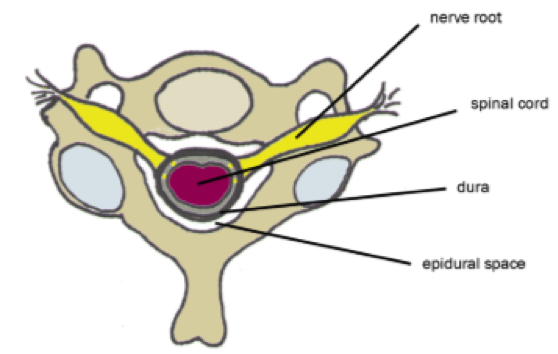
An epidural is regional anesthesia placed in the epidural space, right next to your spinal cord. The anesthesiologist inserts a needle between your vertebra while you sit with your back arched like a cat. Getting the needle in just the right place is difficult; you will be asked a series of questions and given a test dose to try to check its placement.
The type and amount of medication will vary a lot depending on the doctor or hospital. Buipivicaine is most commonly used, and some doctors add a narcotic.
After the doctor has the needle in the right place, they will insert a catheter (a very flexible, small tube) to replace the needle. This assembly will be taped to your back and go to the IV pole, where the medicine bag is placed. You may be given a button to press to administer more of the drug when you need it, or you may have to call someone.
The part of the procedure where you have to sit still takes about 5-10 minutes, but the time from asking for an epidural to actual labor pain relief can easily take an hour, or longer if the anesthesiologist is busy.
What’s is it Like to Get an Epidural For Labor Pain?
Before you get epidural medication in labor, you will receive about a quart of IV fluids, in an attempt to prevent a drop in blood pressure from the drugs. An electronic fetal monitor will be set in place (if it isn’t already) to monitor the baby’s reaction and well-being. You will also have a bladder catheter, a contraction monitor, and a blood pressure cuff.
When the anesthesiologist is ready to place the epidural needle, you will have to sit very still for a few minutes. You will be required to stay in bed and may be asked to roll over occasionally to take pressure off the baby and/or help his heart rate stabilize. If it works, the intensity of labor will be removed or greatly reduced since you won’t have sensation in the lower part of your body.
Some hospitals offer low-dose or ‘walking epidurals.’ The amount of drug used is lower, so some women can shuffle around with their IV poles.
Are Epidurals For Labor Dangerous?
In general, epidural anesthesia is safe. Medical side effects are usually minimal.
Epidurals are tricky, though. The American Academy of Family Physicians quotes researcher Phillip Bromage:
“Superficially, obstetric anesthesia appears to be a simple field with a limited range of interest, but it is a deceptively demanding subspecialty. Not only are two patients involved in each anesthetic administration, but also the dynamic events of normal labor require that the muscles concerned with delivery retain their power and coordination to the full.”
It’s important that you’re able to use your body to labor and then push the baby out the birth canal. Complications can occur when you can’t feel the lower part or lower half of your body.
The most likely complication is that the epidural causes a slowing of your labor or pushing. With an epidural, Pitocin use rises 450% and some have trouble pushing effectively, which can lead to tears and cesarean section delivery.
Statistically, epidural use does have negative effects including increasing your chance of a c-section. However, studies with providers who are committed to keeping c-section rates low show that epidurals don’t necessarily increase the cesarean delivery rate.
Here’s a post dedicated to choosing a provider who is best for you.
When an epidural is used, babies are way more likely to be posterior– to be unable to do the usual rotation so the back of baby’s head is facing your belly. Especially when the epidural is placed early in labor, babies are more likely to have trouble in active labor. Perhaps because of your limited movement, the epidural makes it hard for baby to turn. Posterior babies can be born by vaginal delivery, it is usually just more difficult.
Can an Epidural in Labor Hurt the Baby?
Usually, babies born under the influence of epidural in labor are often ok.
However, the manufacturers of bupivacaine, the most common epidural drug, say “Local anesthetics rapidly cross the placenta and…can cause varying degrees of maternal, fetal, and neonatal toxicity….Adverse reactions in the parturient, fetus, and neonate involve alternations of the central nervous system, peripheral vascular tone, and cardiac function.”
In labors where the mother has had an epidural placed for a long time, the hospital staff calls the NICU team to be on hand in case the baby is born unresponsive.
What are the Risks to Epidural For Labor Pain?
It might not work. The failure rate of epidurals is 12%, though just under half of these are easily fixed and then subsequently provide effective pain relief.
About 5-8% of epidurals have unexplained “windows,” spots on the body where the anesthesia doesn’t take effect.
Epidurals decrease your chance of a vaginal birth and increase your chances of a cesarean delivery (c-section).
Epidural Risks For You Include:
- Restlessness/Anxiety
- Nausea/Vomiting/Chills
- Complications leading to Cesarean
- Developing a fever (1/7)
- Fluid overload from IV
- Increased vaginal tearing
- Forceps/Vacuum extraction
- Temporary urinary incontinence
- Nerve injury or Nerve damage
- Muscle Weakness (1/250)
- Dangerous drop in blood pressure
- Long-term back problems
Serious Effects (Usually From Mistakes):
- Spinal headache (4/1000)
- Convulsions
- Cardiac arrest (1/3000)
- Respiratory distress (1/3000)
Epidural Risks for the Baby:
- Drops in heart rate (distress)
- Low oxygen (blood) to baby
- Forceps/Vacuum extraction
- Low muscle tone
- NICU stay postpartum
- May impact baby’s ability to breastfeed well
What are the Benefits of Epidural For Labor Pain?
When it works, it allows you to relax and let your body labor.
If you are too tense to labor effectively, an epidural will allow you to release that tension and get the baby out.
Your mind and body are one. So if your mind tells your body “I can’t do this. I want it to stop,” your body will listen. You can stop your labor with your mind. When this happens, if you can’t get the support you need to relax and feel confident again, drugs can do that.
If you feel you aren’t coping well and running a lot of stress hormones, an epidural can prevent an excess of stress hormones from affecting your baby.
If you’ve been in labor for an unusually long time and you are too tired to go on, an epidural can help you get some sleep before pushing . So in this way, an epidural may increase your chances for a vaginal birth and prevent a possible cesarean section.
Should I Get an Epidural For Labor Pain?
It’s a smart idea to plan on laboring as long as you can without an epidural. Labor progresses faster and safer when you can move around and feel.
Because the risks increase with the amount of time spent with the anesthesia, getting into advanced labor without it may spare you or your baby from complications.
If you get to the point where you are ready for an epidural, you can call an epidural for labor pain.
Only you can make the decision. It’s important that you don’t make a decision based on feeling pressured by the hospital staff to get an epidural for their comfort. Also, don’t be pressured by your own feelings of guilt over not having a natural birth.
A good provider, your partner or your doula can help you make the epidural in labor decision for pain management when the time comes, and may also help you feel strong enough to not need one. Here is a post dedicated to how a doula can help you in labor.
Disclaimer: Pregnancy by Design’s information is not a substitute for professional medical advice or treatment. Always ask your healthcare provider about any health concerns you may have.
Cited Research
American College of Obstetricians and Gynecologists (2017). Obstetric analgesia and anesthesia. Practice Bulletin No. 177. Obstet Gynecol; 129:e73 – 89. Retrieved from http://journals.lww.com/greenjournal/Abstract/2017/04000/Practice_Bulletin_No__177_Summary___Obstetric.39.aspx
Crawford, JS (1985). Some maternal complications of epidural analgesia for labor. Retrieved from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/4083452.
Gribble, RK and Meier, PR (1991). Effect of epidural analgesia on the primary cesarean rate. Retrieved from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/2067767.
Howell, CJ (1997). Randomised study of long term outcome after epidural versus non-epidural analgesia during labour. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12183305
Lieberman, E. et al. (1997) Epidural analgesia, intrapartum fever, and neonatal sepsis evaluation. Retrieved from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/9041298.
Loftus, JR., Hill, H., and Cohen, SE. (1995) Placental transfer and neonatal effects of epidural sufentanil and fentanyl administered with bupivacaine during labor. Retrieved from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/7631952.
MacArthur, C. Lewis, M., and Knox, EG. (1992). Long term problems after obstetric epidural anaesthesia. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1883505/.
Pan, PH et al. (2004). Incidence and characteristics of failures in obstetric neuraxial analgesia and anesthesia. Retrieved from PubMed https://www.ncbi.nlm.nih.gov/pubmed/15477051.
Philipsen, T. and Jensen NH. (1989). Epidural block or parenteral pethidine and analgesic in labor. Retrieved from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/2924990.
Ramin, SM et al. (1995). Randomized trial of epidural versus intravenous analgesia during labor. Retried from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/7566849.
Thorp, JA and Breedlove, G. (1996). Epidural analgesia in labor: an evaluation of risks and benefits. Retried from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/8826170.
Thorp, JA et al. (1993). The effect of intrapartum epidural analgesia on nulliparous labor: a randomized, controlled, prospective trial. Retried from PubMed at https://www.ncbi.nlm.nih.gov/pubmed/8238138.
 What Is a Birth Plan?
What Is a Birth Plan?






Leave a Reply